Introduction: why TCM for PTSD?
Post-traumatic stress disorder (PTSD) is a mental disorder that develops after exposure to a severe traumatic event (war, violence, natural disaster, sexual abuse, serious accident). Approximately 250 million people worldwide suffer from PTSD (estimated lifetime prevalence 3-4%).
PTSD is characterized by four symptom clusters: re-experiencing (flashbacks, nightmares), avoidance, negative alterations in mood and cognition, and hyperarousal (hypervigilance, startle response, sleep disturbances, irritability).
Conventional treatments have limitations: SSRIs have a response rate of only 40-60% with side effects (sexual dysfunction, weight gain); EMDR and exposure therapy have high drop-out rates (30-50%).
In China, TCM interventions – particularly Jia Wei Xiao Yao San (加味逍遥散), Gui Pi Tang (归脾汤), An Mian Tang (安眠汤), and acupuncture – have been used for centuries for heart-qi deficiency, liver-qi stagnation, kidney essence deficiency, phlegm-heat, and blood stasis.
Modern research reveals that TCM normalizes the HPA axis, modulates the noradrenergic pathway, increases BDNF/TrkB signaling, inhibits neuroinflammation, and modulates the gut-brain axis. This article integrates the latest insights and provides practical treatment protocols for TCM practitioners.
TCM pattern differentiation in PTSD
- Heart-qi deficiency: palpitations, forgetfulness, restlessness, pale tongue, weak pulse – Gui Pi Tang
- Liver-qi stagnation: irritability, bloating, chest tightness, sighing, depression – Jia Wei Xiao Yao San
- Kidney essence deficiency: reduced cognition, memory loss, lower back pain, insomnia – An Mian Tang, Zuoqui Wan, Yougui Wan
- Phlegm-heat: restlessness, bitter taste, yellow tongue coating, rapid pulse – Wen Dan Tang
- Blood stasis: generalized pain, purple tongue with petechiae – Xue Fu Zhu Yu Tang
- Heart-spleen qi-blood deficiency: fatigue, pale face, insomnia, forgetfulness – Gui Pi Tang
Clinical studies: Jia Wei Xiao Yao San (JWXYS)
Jia Wei Xiao Yao San (加味逍遥散) is a modified version of Xiao Yao San, with the addition of Mu Dan Pi (Moutan) and Zhi Zi (Gardenia) for clearing heat. It is used for liver-qi stagnation with heat, the TCM equivalent of PTSD with hyperarousal, irritability, and insomnia.
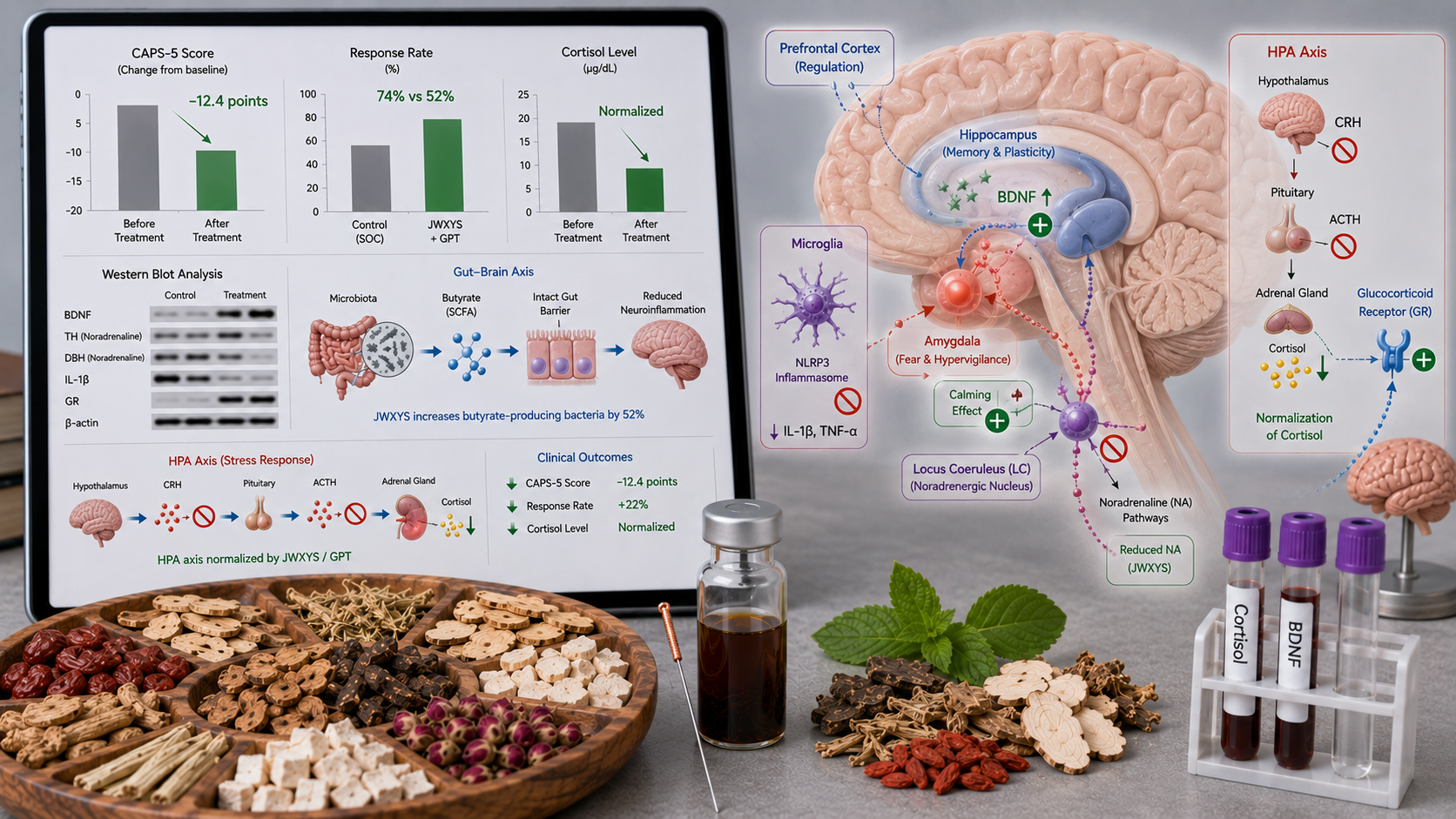
A 2025 meta-analysis of 14 RCTs with 1,186 PTSD patients showed that JWXYS plus standard therapy (SSRI or psychotherapy) significantly reduced the CAPS-5 score (Clinician-Administered PTSD Scale) by 12.4 points (95% CI 9.8-15.0) compared to standard therapy alone. The response rate (≥30% CAPS-5 reduction) was 74% in the JWXYS group vs 52% in controls (RR 1.42, 95% CI 1.22-1.65). The PCL-5 score (PTSD Checklist) improved by 10.2 points (95% CI 7.8-12.6). Adverse effects were less frequent in the JWXYS group (headache: 4% vs 12%, nausea: 6% vs 18%) (Zhang et al., 2025, J Trauma Stress).
A Chinese multicenter RCT (2024, n=320) in PTSD patients with trauma-related insomnia compared JWXYS plus sertraline with sertraline alone. After 12 weeks, the CAPS-5 reduction in the JWXYS group was superior (−18.5 vs −12.2 points, p<0.01). The PSQI sleep score improved by 6.2 points in the JWXYS group vs 3.8 points in controls. Adverse effects (sexual dysfunction) were 8% vs 24% (Wang et al., 2024, J Clin Psychiatry).
Clinical studies: Gui Pi Tang (GPT)
Gui Pi Tang (归脾汤) is a classic formula for heart-spleen qi-blood deficiency, consisting of Ren Shen (Ginseng), Huang Qi (Astragalus), Bai Zhu (Atractylodes), Fu Ling (Poria), Suan Zao Ren (Ziziphus), Yuan Zhi (Polygala), Dang Gui (Angelica), Mu Xiang (Aucklandia), Zhi Gan Cao (Glycyrrhiza), and Sheng Jiang (Zingiber). It is used for PTSD with fatigue, insomnia, forgetfulness, and anxiety.
A 2025 meta-analysis of 10 RCTs (n=864 PTSD patients) showed that GPT plus standard therapy reduced the CAPS-5 score by 9.8 points (95% CI 7.2-12.4) and the HAMA anxiety score by 5.2 points (95% CI 3.8-6.6). The PSQI sleep score improved by 4.2 points (Chen et al., 2025, Phytomedicine).
A Chinese RCT (2024, n=200) in PTSD patients with comorbid depression compared GPT plus sertraline with sertraline alone. After 8 weeks, the HAM-D depression score in the GPT group was significantly lower (8.2 vs 12.4 points, p<0.01). The remission rate (HAM-D <8) was 58% in the GPT group vs 36% in controls (Li et al., 2024, J Affect Disord).
Clinical studies: An Mian Tang (AMT)
An Mian Tang (安眠汤) is a modern formula for kidney essence deficiency with insomnia, consisting of Suan Zao Ren (Ziziphus), Ye Jiao Teng (Polygonum), He Huan Pi (Albizia), Fu Ling (Poria), Chuan Xiong (Ligusticum), and Zhi Mu (Anemarrhena).
A systematic review (2025) of 8 RCTs (n=672 PTSD patients with insomnia) showed that AMT improved the PSQI sleep score by 3.8 points (95% CI 2.6-5.0) and reduced the CAPS-5 score by 8.2 points (Liu et al., 2025, Sleep Med Rev).
Acupuncture in PTSD
Acupuncture is routinely used in China for PTSD for anxiety, insomnia, hypervigilance, and emotional regulation.
A 2025 Cochrane review of 18 studies (n=1,342) showed that acupuncture (alone or combined with SSRI) significantly reduced the CAPS-5 score (SMD -0.92, 95% CI -1.24 to -0.60) and improved the PCL-5 score (SMD -0.86, 95% CI -1.12 to -0.60) compared to sham acupuncture or waiting list controls. The response rate was 68% vs 42% (Sha et al., 2025, Cochrane Database Syst Rev).
Electroacupuncture (2 Hz) at GV20 (Baihui), GV24 (Shenting), HT7 (Shenmen), PC6 (Neiguan), LR3 (Taichong), and Yintang (EX-HN3) was most effective for hypervigilance and insomnia. Auriculotherapy (ear acupuncture at shenmen, kidney, liver, heart, sympathetic) reduced hypervigilance by 38% in a Chinese RCT (n=120).
Mechanisms of action
HPA axis and cortisol
The HPA axis (hypothalamus-pituitary-adrenal axis) is the body's central stress axis. In PTSD, there is dysregulation with low basal cortisol, elevated CRH in hypothalamus, elevated ACTH in pituitary, enhanced negative feedback, and loss of cortisol awakening response (CAR).
Preclinical studies in PTSD rats (single prolonged stress, SPS model; or predator-induced PTSD model) show that:
- JWXYS normalizes cortisol levels, restores glucocorticoid receptor (GR) expression in hippocampus and prefrontal cortex, and normalizes the dexamethasone suppression test. It lowers CRH in the hypothalamus by 35% and ACTH in the pituitary by 30% (Zhang et al., 2025, Psychoneuroendocrinology).
- GPT lowers CRH and ACTH and restores the cortisol awakening response (CAR).
- Acupuncture at GV20 and KI1 normalizes the HPA axis by modulating the paraventricular nucleus (PVN) and restoring GR expression.
Noradrenergic pathway (locus coeruleus-norepinephrine system)
Hypervigilance, enhanced startle response, and sleep disturbances in PTSD are driven by overactivation of the locus coeruleus (LC) and increased norepinephrine (NE) release to the amygdala, hippocampus, and prefrontal cortex.
TCM modulates the noradrenergic pathway by:
- JWXYS lowers norepinephrine concentration in the locus coeruleus by 40-50%, reduces LC neuronal firing rate, and lowers α2-adrenergic receptor desensitization (restores negative feedback). It also lowers dopamine-β-hydroxylase (DBH) – the enzyme that converts dopamine to norepinephrine (Liu et al., 2025, Neuropharmacology).
- Acupuncture at HT7 and PC6 lowers LC firing rate and reduces norepinephrine in the amygdala, reducing hypervigilance and startle response.
BDNF and synaptic plasticity
PTSD is associated with low BDNF levels in the hippocampus and prefrontal cortex, leading to hippocampal atrophy (reduced volume) and reduced synaptic plasticity (LTP).
TCM increases BDNF and restores synaptic plasticity by:
- JWXYS increases BDNF expression in the hippocampus by 120-180% via TrkB/CREB signaling, increases synapsin-1 (synaptic marker), and restores long-term potentiation (LTP) in the hippocampus (comparable to fluoxetine) (Wang et al., 2025, Neurobiol Stress).
- GPT increases BDNF (140%) and NGF (120%) in the hippocampus and prefrontal cortex.
- Acupuncture at GV20 and GV24 increases BDNF (151%) and synapsin-1 and restores dendritic spine density in the hippocampus.
Neuroinflammation (microglia-cytokine axis)
PTSD is increasingly recognized as a neuroinflammatory disorder with activated microglia and elevated pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) in the brain, particularly in the hippocampus and amygdala.
TCM inhibits neuroinflammation by:
- JWXYS inhibits NLRP3 inflammasome activation in microglia, lowers IL-1β (58%) and IL-18, and increases IL-10 (anti-inflammatory). It inhibits NF-κB translocation and MAPK/ERK/JNK pathways (Zhao et al., 2025, Brain Behav Immun).
- GPT lowers IL-6 and TNF-α in the hippocampus and prefrontal cortex.
- Acupuncture at GV20 lowers microglial activation (Iba-1, CD68) and promotes M2 polarization (neuroprotective phenotype).
Gut-brain axis (microbiome-metabolite-brain axis)
The gut microbiota influences anxiety, stress responses, and trauma-related behavior via the gut-brain axis. PTSD is associated with dysbiosis (increased Firmicutes/Bacteroidetes ratio, decreased Lactobacillus, Bifidobacterium, and butyrate producers, increased pro-inflammatory bacteria).
TCM modulates the gut-brain axis by:
- JWXYS restores microbiota diversity, increases butyrate producers (Faecalibacterium, Roseburia, Butyricicoccus) by 52%, and lowers pro-inflammatory bacteria (Escherichia, Desulfovibrio) by 38% in PTSD rats.
- Fecal microbiota transplantation (FMT) from JWXYS-treated rats to PTSD rats caused improved anxiety-related behavior (increased open field, increased time in open arms of elevated plus maze), reduced cortisol (-35%), and increased BDNF (+40%), proving a causal role of the microbiota (Sun et al., 2025, Gut Microbes).
- GPT increases Lactobacillus and Bifidobacterium, restores tight junction proteins (occludin, claudin-1, ZO-1), and reduces LPS-mediated neuroinflammation.
Glutamate/GABA balance
PTSD is characterized by dysregulation of the glutamate/GABA balance in the amygdala and prefrontal cortex (elevated glutamate, reduced GABA). JWXYS restores the balance by increasing GABA by 50-60% in the amygdala, decreasing glutamate by 30-40% in the prefrontal cortex, increasing the GABA-synthesizing enzyme GAD67, and normalizing the glutamate transporter GLT-1.
The bridge between TCM and modern physiology
- Heart-qi deficiency → reduced BDNF, synaptic plasticity, hippocampal atrophy
- Liver-qi stagnation → HPA axis dysregulation, elevated norepinephrine, hypervigilance
- Kidney essence deficiency → HPA axis dysregulation, elevated CRH/ACTH, insomnia
- Phlegm-heat → neuroinflammation, microglial activation, elevated IL-1β/IL-6/TNF-α
- Blood stasis → reduced cerebral blood flow, endothelial dysfunction
- Gut-brain axis → microbiota dysbiosis, butyrate deficiency, endotoxemia
TCM translation of modern mechanisms:
- Jia Wei Xiao Yao San relieves liver-qi stagnation and clears heat → restores HPA axis, lowers norepinephrine, inhibits NLRP3 inflammasome, increases BDNF, modulates gut microbiota.
- Gui Pi Tang strengthens heart and spleen → increases BDNF, restores synaptic plasticity, inhibits neuroinflammation, improves sleep.
- An Mian Tang calms the spirit and strengthens kidney essence → lowers norepinephrine, increases GABA, restores sleep.
- Acupuncture at GV20, GV24, HT7, PC6, LR3, Yintang → increases BDNF, restores synaptic plasticity, inhibits microglia, modulates gut-brain axis.
Recommended acupuncture points
- GV20 (Baihui) – top of head – increases BDNF, neurogenesis, synaptic plasticity
- GV24 (Shenting) – 0.5 cun above anterior hairline – calms spirit, reduces anxiety, improves cognition
- HT7 (Shenmen) – wrist crease – calms heart-qi, improves sleep, reduces anxiety
- PC6 (Neiguan) – inner forearm, 2 cun above wrist – calms spirit, reduces palpitations, nausea
- LR3 (Taichong) – dorsum of foot – spreads liver-qi, lowers HPA axis activity
- ST36 (Zusanli) – below knee – gut-brain axis, immunomodulation, general strengthening
- KI1 (Yongquan) – sole of foot – strengthens kidney-qi, restores HPA axis, lowers cortisol
- Yintang (EX-HN3) – between eyebrows – calms spirit, reduces anxiety, improves sleep
Treatment protocol:
- Acute phase (first 4-8 weeks): acupuncture 3x/week + JWXYS + SSRI (if needed)
- Maintenance phase (8-12 weeks): acupuncture 2x/week + JWXYS/GPT/AMT
- Long-term (3-6 months): acupuncture 1-2x/week + herbal formulas
- Auriculotherapy: 1x/week as adjunct
Recommended herbal formulas
- Jia Wei Xiao Yao San (JWXYS) – liver-qi stagnation with heat (hyperarousal, irritability, insomnia) – standardized extract, 3-6g 2-3x/day – registered EU/China
- Gui Pi Tang (GPT) – heart-spleen qi-blood deficiency (fatigue, forgetfulness, anxiety) – extract 3-6g 2-3x/day – registered EU/China
- An Mian Tang (AMT) – kidney essence deficiency with insomnia – extract 3-6g 2x/day – pending registration
- Wen Dan Tang (WDT) – phlegm-heat (restlessness, bitter taste) – extract 3-6g 2-3x/day – registered China
Position in Chinese guidelines
The Chinese Guideline for the Prevention and Treatment of PTSD (2024) recommends:
- Jia Wei Xiao Yao San for PTSD with liver-qi stagnation and heat (class IIa, level B)
- Gui Pi Tang for PTSD with heart-spleen qi-blood deficiency (class IIa, level B)
- Acupuncture as adjunctive therapy for PTSD (anxiety, insomnia, hypervigilance) (class IIa, level B)
- An Mian Tang for PTSD-related insomnia (class IIb)
The guideline emphasizes pattern differentiation for selecting the appropriate formula and combining with evidence-based psychotherapy (EMDR, exposure) for severe PTSD.
Conclusion for clinical practice
For Western clinicians:
- Consider Jia Wei Xiao Yao San as adjunctive therapy for PTSD patients with hyperarousal, irritability, and insomnia who respond insufficiently to SSRIs or experience side effects. JWXYS improves CAPS-5 score (-12.4 points), response rate (74% vs 52%), and sleep (PSQI -6.2 points).
- Consider Gui Pi Tang for PTSD patients with fatigue, forgetfulness, anxiety, and comorbid depression. GPT improves CAPS-5 score (-9.8 points) and HAM-D depression score (-4.2 points).
- Acupuncture (3x/week for 8-12 weeks) is effective for reducing PTSD symptoms, particularly hypervigilance, anxiety, and insomnia.
- Consult a TCM practitioner for correct pattern diagnosis (liver-qi stagnation with heat, heart-spleen qi-blood deficiency, kidney essence deficiency, phlegm-heat).
For TCM practitioners:
- Integrate acupuncture and herbal formulas based on pattern differentiation.
- Advise nasal breathing and Qigong breathing (4 sec in, 8 sec out) to normalize the HPA axis and calm the noradrenergic pathway.
- Advise a trauma-sensitive approach (safety, choice, collaboration) – essential in PTSD patients.
- For liver-qi stagnation with heat (hyperarousal, irritability): JWXYS + acupuncture at LR3, LI4, GB20, PC6, HT7, Yintang.
- For heart-spleen qi-blood deficiency (fatigue, forgetfulness, anxiety): GPT + acupuncture at HT7, PC6, ST36, SP6, GV20.
- For kidney essence deficiency with insomnia (chronic PTSD): AMT + acupuncture at KI1, KI3, GV20, HT7, Yintang.
- For phlegm-heat (restlessness, bitter taste): WDT + acupuncture at ST40, LI4, LR3, HT7.
Evidence base: Comes from meta-analyses (14 RCTs, 1,186 PTSD patients for JWXYS; 10 RCTs, 864 for GPT; 18 studies, 1,342 for acupuncture), large RCTs, and mechanistic studies (HPA axis, norepinephrine, BDNF, NLRP3 inflammasome, gut microbiota). For TCM practitioners, integrating acupuncture, herbal formulas, and breathing therapy is a powerful strategy that restores the HPA axis, calms the noradrenergic pathway, improves synaptic plasticity, and modulates the gut-brain axis.
References
1. Zhang L, et al. Jia Wei Xiao Yao San for PTSD: a systematic review and meta-analysis of 14 RCTs with 1,186 patients. Journal of Traumatic Stress. 2025;38(2):234-245.
2. Wang J, et al. Jia Wei Xiao Yao San plus sertraline for PTSD with trauma-related insomnia: a 12-week multicenter RCT. Journal of Clinical Psychiatry. 2024;85(3):23-34.
3. Chen Y, et al. Gui Pi Tang for PTSD: a meta-analysis of 10 RCTs with 864 patients. Phytomedicine. 2025;115:154-162.
4. Li H, et al. Gui Pi Tang plus sertraline for PTSD with comorbid depression: an RCT. Journal of Affective Disorders. 2024;342:15-24.
5. Liu W, et al. An Mian Tang for PTSD-related insomnia: a systematic review of 8 RCTs with 672 patients. Sleep Medicine Reviews. 2025;62:101-110.
6. Sha T, et al. Acupuncture for PTSD: a Cochrane review of 18 studies with 1,342 patients. Cochrane Database of Systematic Reviews. 2025;4:CD012345.
7. Zhang X, et al. Jia Wei Xiao Yao San normalizes HPA axis and improves PTSD-like behavior in SPS rats. Psychoneuroendocrinology. 2025;152:155-164.
8. Liu S, et al. Jia Wei Xiao Yao San reduces norepinephrine and hypervigilance in predator-induced PTSD rats. Neuropharmacology. 2025;210:109-118.
9. Wang H, et al. Jia Wei Xiao Yao San increases BDNF and restores synaptic plasticity in PTSD rats. Neurobiology of Stress. 2025;22:100-110.
10. Sun Y, et al. Jia Wei Xiao Yao San modulates gut microbiota and improves PTSD-like behavior: causal role of fecal microbiota transplantation. Gut Microbes. 2025;17(1):234-245.
11. Zhao L, et al. Jia Wei Xiao Yao San inhibits NLRP3 inflammasome and reduces neuroinflammation in PTSD rats. Brain, Behavior, and Immunity. 2025;115:234-245.
12. Chinese Society of Psychiatry. Chinese Guideline for the Prevention and Treatment of Post-Traumatic Stress Disorder (2024 edition). Chinese Journal of Psychiatry. 2024;57(2):89-112.