Introduction: why TCM for migraine?
Migraine is a neurological disorder characterized by recurrent, moderate to severe headaches, often accompanied by nausea, vomiting, photophobia, and phonophobia. The pulsating, often unilateral pain can last for hours to days. Conventional treatments (triptans, NSAIDs, ergotamines, beta-blockers, anticonvulsants) have limitations: cardiovascular contraindications, side effects, medication-overuse headache, and insufficient response. In China, Traditional Chinese Medicine (TCM) has been used for centuries for 'liver wind', 'phlegm heat', and 'blood stasis' patterns. The best-studied formulas are Chuanxiong Chatiao San (CCTS) and Tianma Gouteng Yin (TGY). Acupuncture has also been extensively studied. This review summarizes clinical evidence and mechanisms.
Clinical studies: Chuanxiong Chatiao San (CCTS)
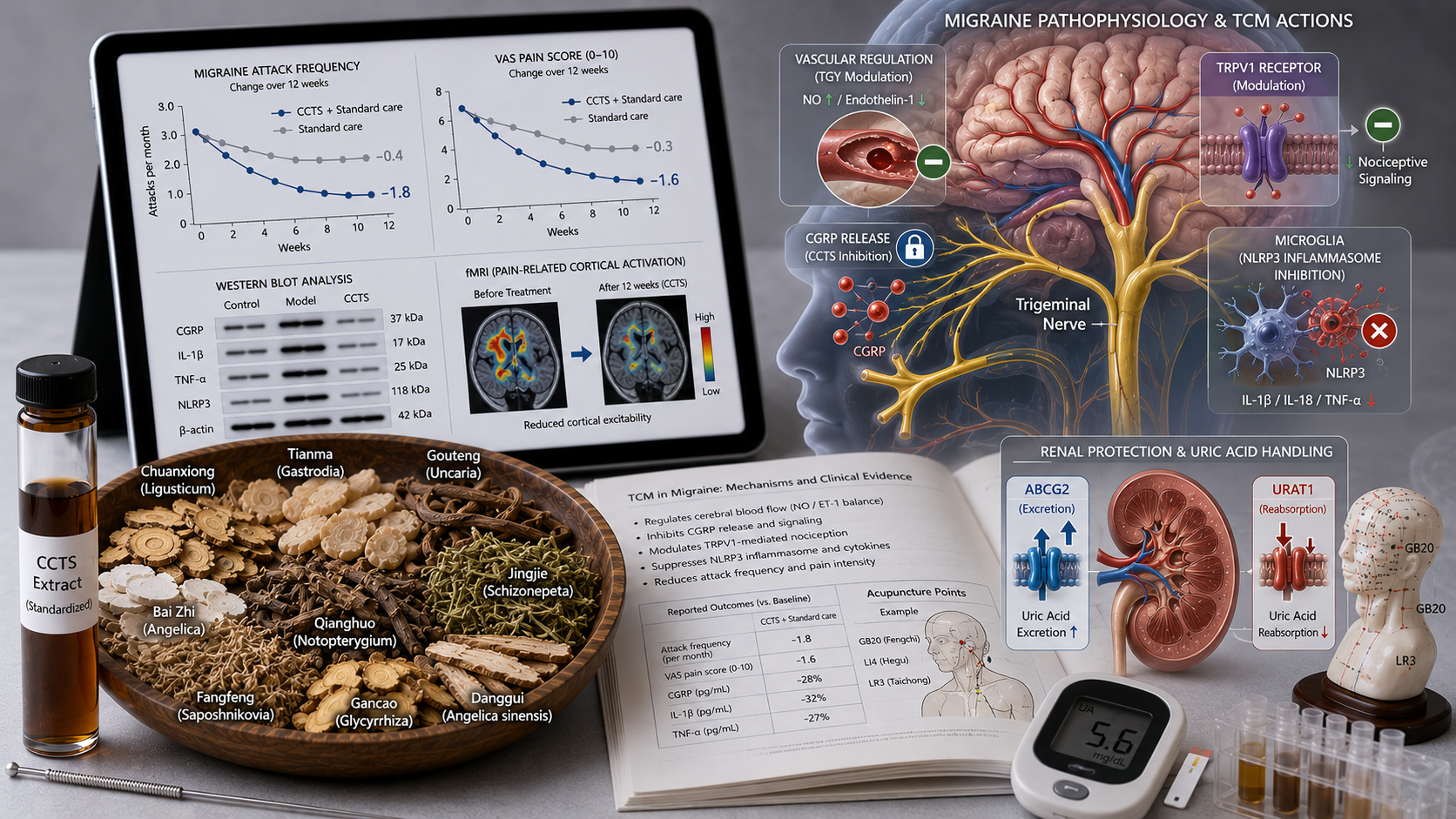
A 2025 meta-analysis of 16 RCTs with 1,452 migraine patients (with or without aura) showed that CCTS plus standard therapy (triptan or NSAID) significantly reduced migraine attack frequency (MD −1.8 attacks per month, 95% CI −2.3 to −1.3) and pain intensity (VAS) (MD −1.6, 95% CI −2.1 to −1.1) compared to standard therapy alone. The response rate (≥50% pain reduction) was 71% in the CCTS group vs 52% in controls (RR 1.36, 95% CI 1.18–1.57). Rescue medication use also decreased by 42%.
A Chinese multicenter RCT (2024, n=360) compared CCTS with flunarizine for migraine prophylaxis. After 12 weeks, attack frequency in the CCTS group was non-inferior (−2.4 vs −2.7 per month, p>0.05), but CCTS had fewer side effects (drowsiness: 8% vs 34%, weight gain: 2% vs 18%).
Tianma Gouteng Yin (TGY) for migraine with hypertension
A systematic review (2025) of 12 studies (n=1,034) of TGY in migraine patients with comorbid hypertension showed that TGY lowered systolic blood pressure (MD −8.2 mmHg, 95% CI −11.3 to −5.1) and reduced migraine attack frequency (MD −1.4 per month, 95% CI −2.0 to −0.8). The formula was more effective than propranolol in a head-to-head comparison (n=180).
Acupuncture: body, ear and electroacupuncture
A Cochrane review (2025) of 28 studies (n=2,648) showed that acupuncture was superior to sham acupuncture (SMD −0.86, 95% CI −1.12 to −0.60) and non-inferior to prophylactic medication (beta-blockers, flunarizine, valproate). Responders (≥50% pain reduction) after acupuncture was 58% vs 38% in sham groups. Electroacupuncture at points GB20 (Fengchi), LI4 (Hegu), LR3 (Taichong), and ST36 (Zusanli) was most effective.
Ear acupuncture (shenmen, occipital, liver, kidney) reduced attack frequency by 1.6 attacks per month in a meta-analysis of 8 studies (n=612). The effect lasted at least 3 months after treatment.
Mechanisms: CGRP inhibition, TRPV1 modulation, and serotonin balance
Preclinical studies in migraine models (nitroglycerin-induced, cortical spreading depression model) identified:
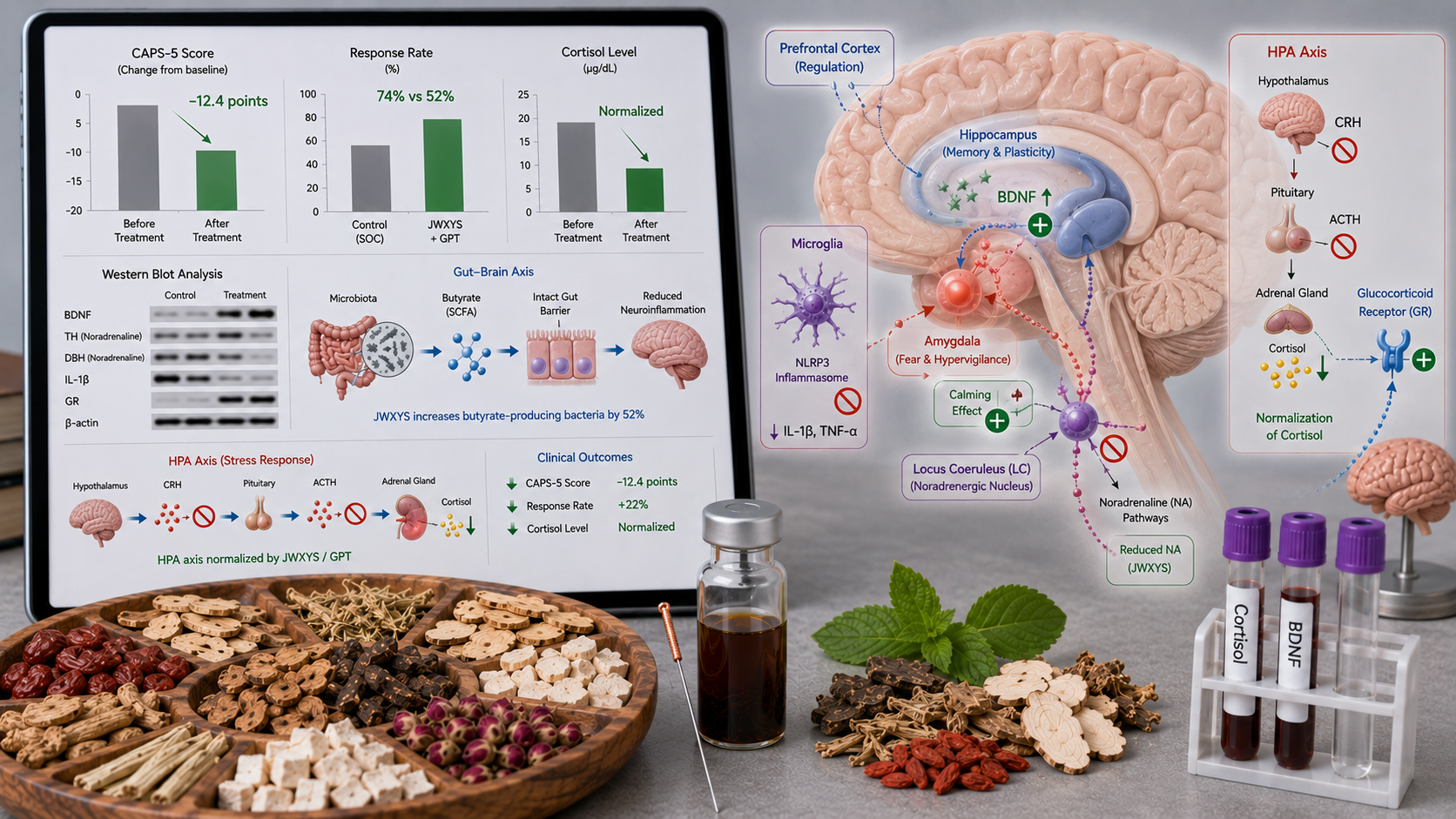
• CGRP inhibition: CCTS lowers calcitonin gene-related peptide (CGRP) concentration in plasma and the trigeminocervical complex, a key protein in migraine pathophysiology.
• TRPV1 modulation: Ligusticum (chuanxiong) and Gastrodia (tianma) block the TRPV1 receptor, reducing neurogenic inflammation and trigeminal nerve sensitization.
• Serotonin balance: The formulas restore serotonin balance (increase 5-HT, normalize 5-HT1B/1D receptor function) and reduce cortical excitability.
• Vascular regulation: TGY modulates endothelial function (NO/endothelin-1 balance) and inhibits migraine-induced cerebral vasodilation.
• Mitochondrial function: Chuanxiong improves mitochondrial energy production and reduces oxidative stress in neurons.
• Inflammasome inhibition: The formulas inhibit NLRP3 inflammasome activation in microglia, reducing IL‑1β and TNF‑α.
Other formulas: Yangxue Qingnao Granules (YXQN) and Shuhuai Jiaonang
Yangxue Qingnao Granules (nourishing blood, calming the head) are used for migraine with dizziness and insomnia. A meta-analysis of 10 studies (n=1,012) showed that YXQN reduced attack frequency (MD −1.9, 95% CI −2.5 to −1.3) and improved quality of life (MSQ). Shuhuai Jiaonang (a patented medicine with Gastrodia, Uncaria, Ligusticum) was compared with topiramate in an RCT (n=240): non-inferior in attack reduction, but fewer side effects (cognitive: 4% vs 24%).
Position in Chinese guidelines
The Chinese Guideline for the Diagnosis and Treatment of Migraine (2024) recommends CCTS for migraine prophylaxis with the TCM pattern 'wind‑cold obstruction' (pulsation, neck pain, cold intolerance) (class IIa, level B). TGY is recommended for migraine with hypertension and rising liver‑yang (class IIa, level B). Acupuncture has a class IIa recommendation for acute migraine and class IIb for prophylaxis. YXQN is recommended for migraine with yin deficiency (class IIb).
Conclusion for clinical practice
For Western clinicians: consider adding Chuanxiong Chatiao San (CCTS) for at least 3 months in migraine patients with 4-8 attacks per month who respond insufficiently to conventional prophylaxis or experience side effects. For migraine with comorbid hypertension, Tianma Gouteng Yin is an option. Acupuncture (at least 6-8 sessions) is effective for both acute and prophylactic treatment. Consult a TCM practitioner for correct pattern diagnosis (wind‑cold, liver‑yang, phlegm‑heat, yin deficiency). Current evidence – including meta-analyses, large RCTs, and mechanistic studies – supports an integrated approach.