Introduction: why TCM for insomnia?
Chronic insomnia affects 10–30% of adults worldwide and leads to reduced cognition, increased risk of anxiety/depression, and lower quality of life. Current drugs (benzodiazepines, Z‑drugs) often cause adverse effects such as drowsiness, tolerance, and dependence. In China, TCM herbal formulas and acupuncture have been routinely used for centuries. The best‑studied intervention is SuanZaoRen Tang (SZRT), a classic formula from the Jingui Yaolue, intended for insomnia due to liver‑blood deficiency. This review summarizes clinical evidence and mechanisms.
Clinical studies: SuanZaoRen Tang and Jiawei SuanZaoRen Tang
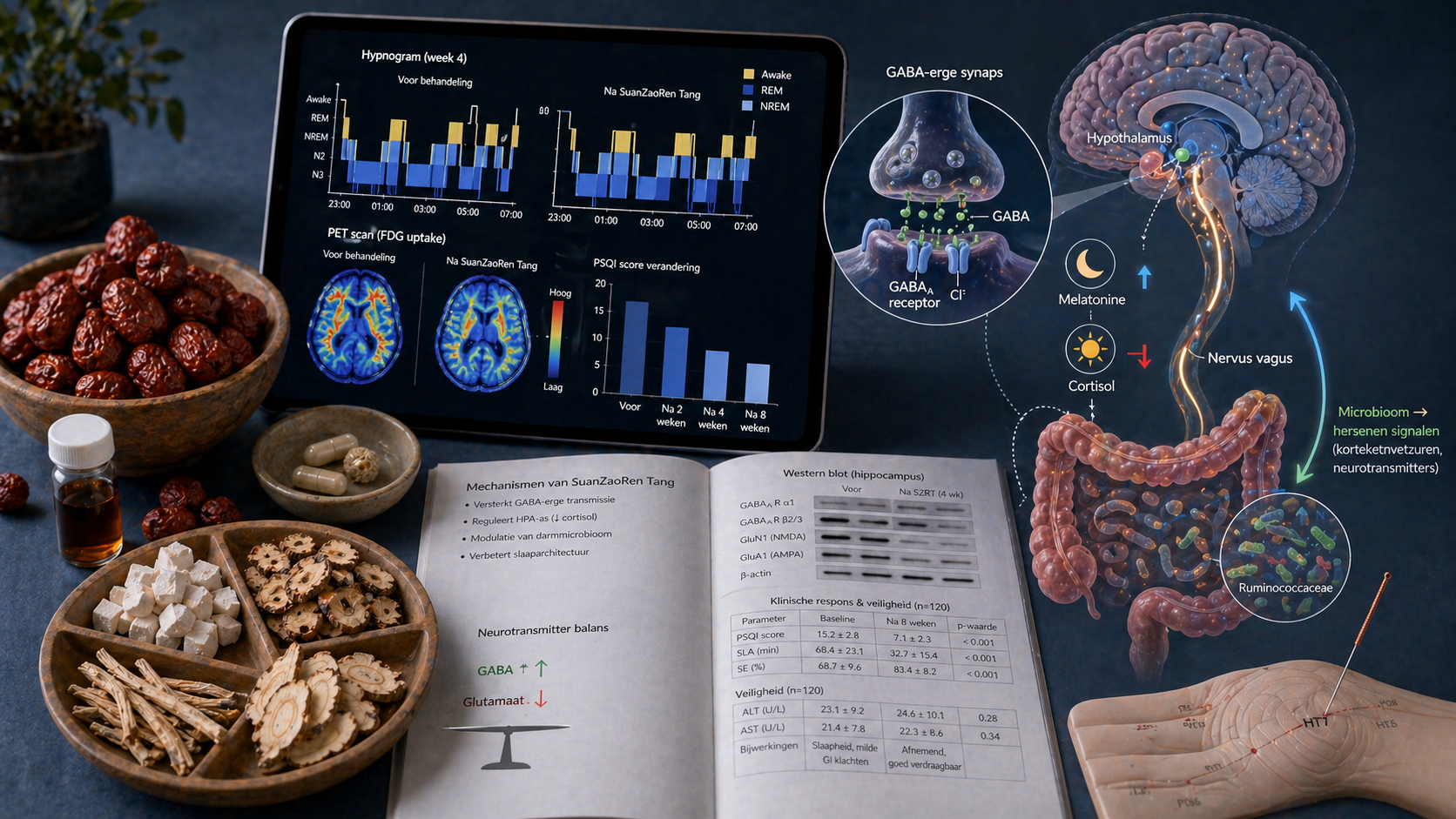
A comprehensive meta‑analysis (2025) of 32 RCTs with a total of 2,845 patients showed that SZRT significantly reduced PSQI score (MD −2.89, 95% CI −3.42 to −2.36) without serious adverse events. An fMRI study (2025) in 82 chronic insomnia patients demonstrated improved sleep efficiency and cognitive function, with measurable changes in regional brain activity (ReHo) correlating with clinical improvement. In perimenopausal insomnia (80 patients), Jiawei SuanZaoRen Tang (JW‑SZRT) was as effective as lorazepam, but with a better hormonal profile (increase in estradiol, decrease in FSH/LH) and increased 5‑HT and GABAA receptors in the hypothalamus. Response rate was 78% in the JW‑SZRT group vs 54% in controls (p<0.01).
Acupuncture: effects on sleep quality and the endocrine system
A meta‑analysis of 12 RCTs (n=1,012) showed that acupuncture significantly improves PSQI (MD −3.39, 95% CI −4.20 to −2.59) and also lowers ISI in sham‑controlled studies (MD −1.82, 95% CI −2.95 to −0.68). Notably, endocrine modulation: acupuncture raises serum melatonin (MD +5.29 pg/ml) and reduces salivary cortisol (MD −0.05 μg/dL). In addition, acupuncture improves daily cognition and fatigue, as shown in a meta‑analysis of 18 studies (n=1,767). An RCT (76 patients) showed that acupuncture at points HT7, BL15, LR3, and BL18 reduced anxiety and depression scores (BAI/BDI) significantly more than a control point set (p<0.05).
Mechanisms: from GABA to gut microbiota
An animal study (2025) in a PCPA‑induced insomnia model showed that SZRT:
• **Restores GABA/glutamate balance**: GABA increased, glutamate decreased in the brain.
• **Suppresses neuroinflammation**: IL‑6, TNF‑α, and CYP2E1 decreased, with restoration of GFAP and Iba‑1 expression in glial cells.
• **Modulates the gut microbiota**: The decline in Prevotellaceae and Butyricicoccus was corrected, with effects on branched‑chain amino acids and inflammatory pathways. These findings support the microbiome‑metabolite‑brain axis.
• **Synaptic plasticity**: In a comorbid anxiety model (2026), the Zhi‑Gan formula restored PACAP-eEF2-BDNF signaling in the medial prefrontal cortex, improving long‑term potentiation (LTP).
Furthermore, a human study (2024) with 63 insomnia patients and two distinct TCM syndromes showed that microbiome composition differs between syndromes, and syndrome‑specific formulas improved sleep within two weeks. Longitudinal network analysis revealed connections between sleep quality, gut bacteria (e.g., Phascolarctobacterium and Ruminococcaceae), and inflammatory markers.
Position in Chinese guidelines
The Chinese Guideline for the Diagnosis and Treatment of Insomnia (2023) recommends TCM herbs for specific patterns: SuanZaoRen Tang for liver‑blood deficiency, GuiPi Tang for spleen‑heart qi‑blood deficiency, and Jiaotai Pill for kidney‑heart imbalance (all class IIa, level B). Acupuncture has a class IIa recommendation for chronic insomnia. Guidelines always advise syndrome differentiation before selecting the appropriate intervention.
Conclusion for clinical practice
For Western clinicians: consider SuanZaoRen Tang (or its Jiawei variant) for an insomnia patient with liver‑blood deficiency (restless sleep, dreaminess, fatigue, pale tongue, thin pulse), especially if prior hypnotics worked insufficiently or caused adverse effects. Acupuncture is a well‑substantiated option to improve both night‑time sleep and daily cognition and mood. The evidence comes from double‑blind RCTs, meta‑analyses, and mechanistic studies. Consult a TCM practitioner for correct syndrome diagnosis.