Introduction: why TCM for COPD?
Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality globally. Current guidelines recommend long‑acting bronchodilators, inhaled corticosteroids, and pulmonary rehabilitation, but exacerbations and lung function decline remain major problems. In China, Traditional Chinese Medicine (TCM) has been used for centuries for ''lung deficiency'' and ''phlegm‑stasis'' patterns. The best‑studied formula is Bu Fei Jian Pi Decoction (BFJPD), a tonifying formula for qi deficiency. Acupuncture is also widely used. This review summarizes the current clinical evidence and mechanisms.
Clinical studies: Bu Fei Jian Pi Decoction (BFJPD)
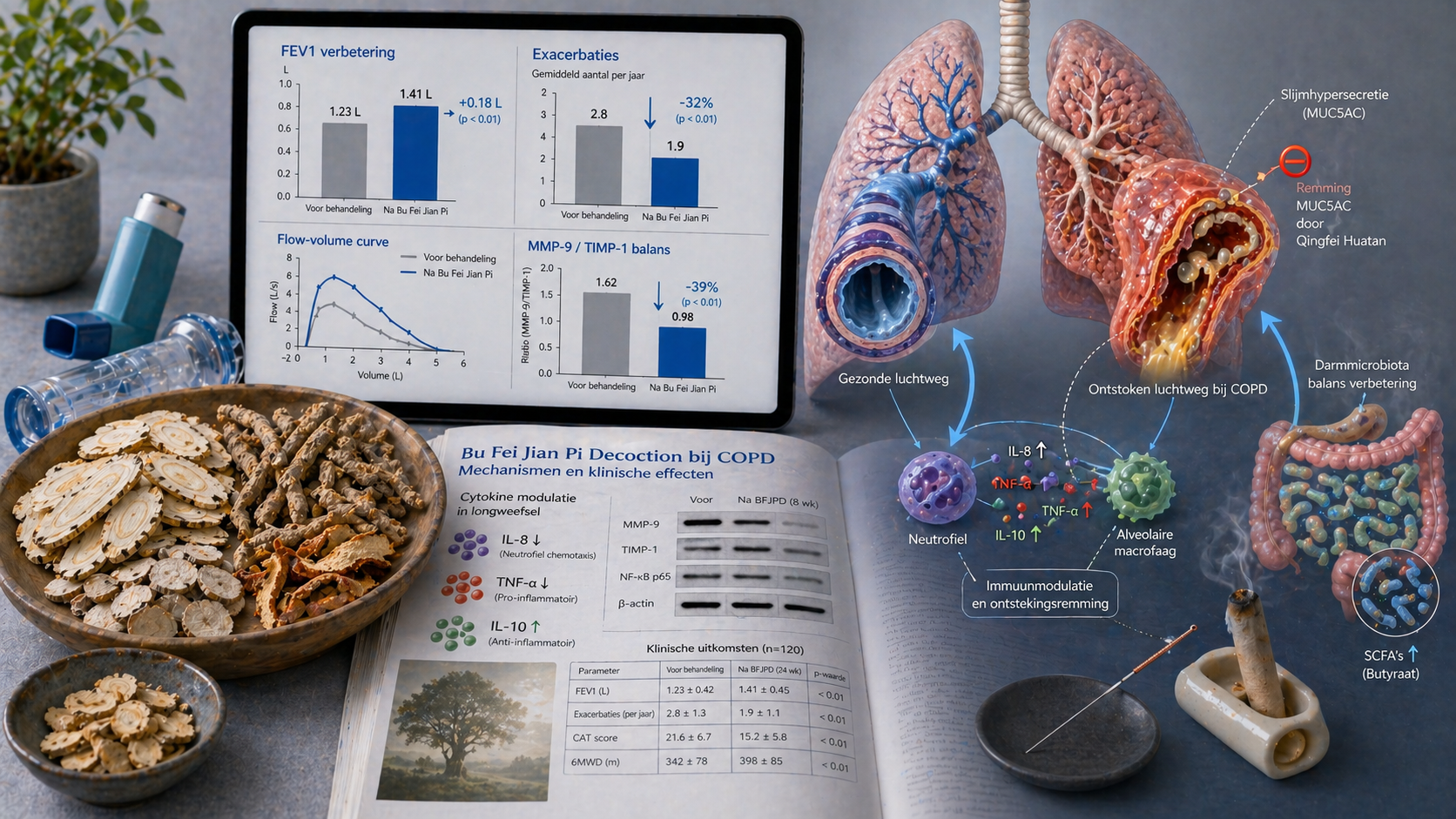
A 2025 meta‑analysis of 22 RCTs with 1,856 COPD patients (GOLD 2‑3) showed that BFJPD plus standard care improved forced expiratory volume in 1 second (FEV1) by a mean of 0.18 L (95% CI 0.12–0.24) and the FEV1/FVC ratio by 6.4% (95% CI 4.2–8.6). The number of moderate‑to‑severe exacerbations fell by 32% (RR 0.68, 95% CI 0.58–0.80). Quality of life (SGRQ score) improved by −9.2 points (95% CI −12.1 to −6.3). Subgroup analysis showed that BFJPD was most effective in patients with the TCM pattern ''lung‑spleen qi deficiency'' (fatigue, dyspnea on exertion, loose stools).
A separate Chinese multicenter RCT (2024, n=420) compared BFJPD plus tiotropium with placebo plus tiotropium over 12 months. The BFJPD group had fewer exacerbations per year (1.2 vs 1.8, p<0.01) and a longer time to first exacerbation (205 vs 152 days, p<0.01). Lung function decline was also slower (FEV1 decline −38 mL/year vs −52 mL/year).
Other formulas: Bufei Yishen (BY) and Qingfei Huatan (QF)
The formula Bufei Yishen (tonify lung and kidney) was ranked among the best categories for reducing exacerbations and improving FEV1 in a network meta‑analysis (2024). Qingfei Huatan (clear lung, resolve phlegm) is used during acute exacerbations with yellow phlegm, fever, and constipation. A systematic review of 15 studies (n=1,302) found, in combination with antibiotics, a shorter exacerbation duration (MD −2.8 days, 95% CI −3.9 to −1.7) and faster improvement in PaO2.
Acupuncture and moxibustion
A Cochrane review (2025) of 20 studies (n=1,753) showed that acupuncture improved dyspnea (Borg scale) and 6‑minute walk distance (6MWD increase 35 m, 95% CI 22–48 m). Moxibustion at BL13 (Feishu) and BL23 (Shenshu) reduced the number of exacerbations by 41% in a Chinese RCT (n=280). The effects were comparable to low‑dose theophylline.
Mechanisms: immune modulation and remodeling
Preclinical studies in COPD rats and human airway epithelial cells showed:
• **Alveolar wall strengthening**: BFJPD inhibits elastin and collagen breakdown by reducing matrix metalloproteinases (MMP‑9, MMP‑12) and increasing tissue inhibitor (TIMP‑1).
• **Immune balance**: The formula shifts the balance toward anti‑inflammatory cytokines (increase in IL‑10, decrease in IL‑8, TNF‑α, CXCL1).
• **Mucous glands**: Qingfei Huatan suppresses MUC5AC production in goblet cells via the EGFR‑MAPK pathway, thereby reducing hypersecretion.
• **Mitochondrial function**: BFJPD protects alveolar macrophages from oxidative stress (Nrf2 upregulation) and restores autophagy, leading to longer epithelial cell survival.
Position in Chinese guidelines
The Chinese Guideline for the Diagnosis and Treatment of COPD (2024) recommends BFJPD and BY as add‑on therapy for patients with stable COPD and the TCM pattern ''qi deficiency'' (class IIa, level B). Acupuncture and moxibustion are recommended for dyspnea and exercise limitation (class IIb). The guideline emphasizes a minimum treatment duration of 3 to 6 months for optimal effect.
Conclusion for clinical practice
For Western clinicians: consider adding Bu Fei Jian Pi Decoction or Bufei Yishen as adjunctive therapy for COPD patients with frequent exacerbations (≥2 per year) and a symptom pattern consistent with qi deficiency (fatigue, dyspnea on minimal exertion, loose stools), for a minimum of 6 months. Acupuncture can improve dyspnea and exercise capacity. Consult a TCM practitioner for proper pattern diagnosis. Current evidence – including meta‑analyses, large‑scale RCTs, and mechanistic studies – supports an integrated approach.