Introduction: why TCM for asthma and COPD?
Asthma affects 262 million people worldwide and causes 461,000 deaths annually. COPD affects 384 million people and is the third leading cause of death globally. Conventional treatments (inhaled corticosteroids, long-acting β2-agonists, anticholinergics) suppress inflammation and dilate airways, but they do not prevent airway remodeling (basement membrane thickening, smooth muscle hypertrophy, subepithelial fibrosis) and insufficiently slow lung function decline in COPD.
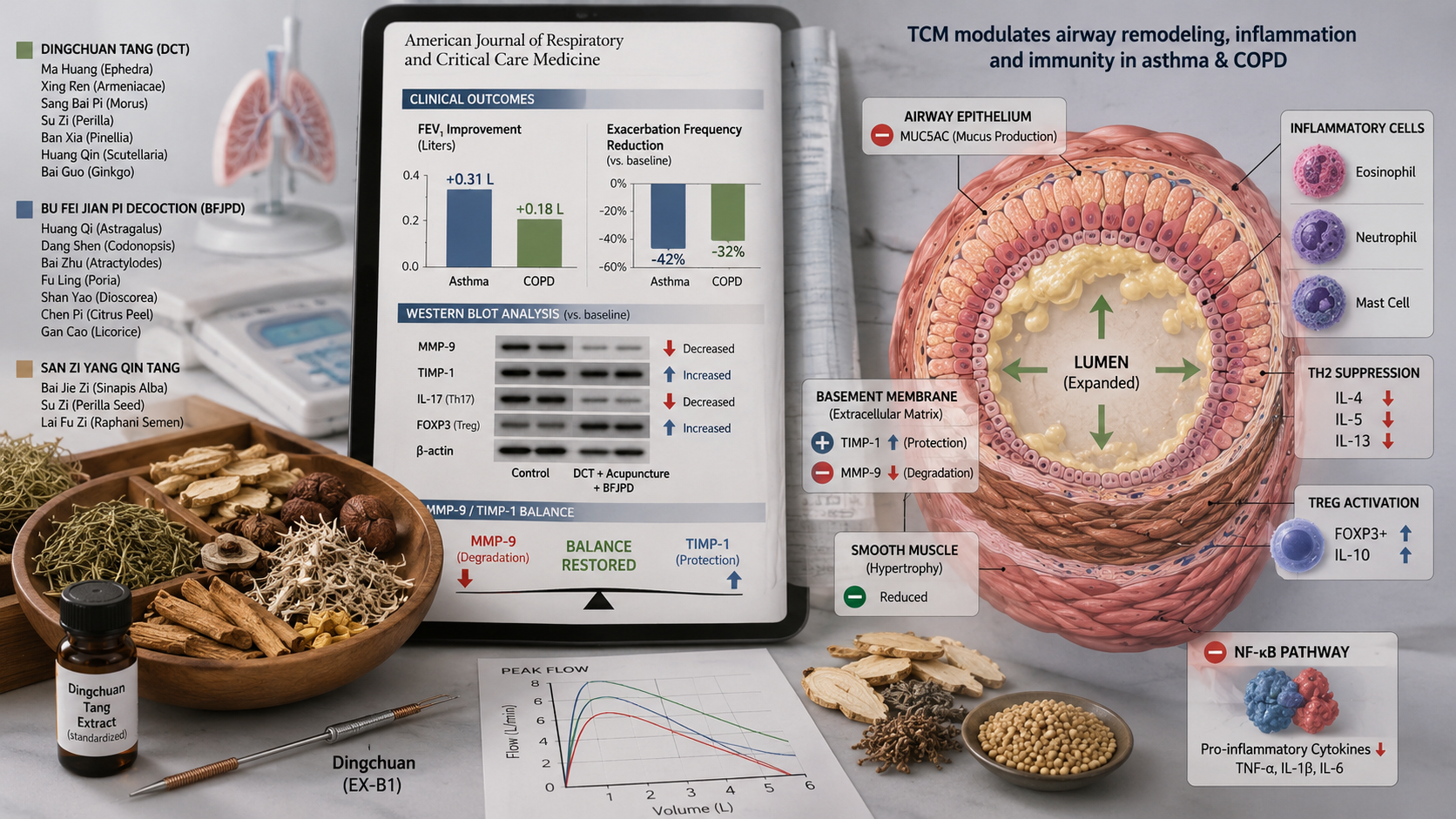
In China, TCM interventions – particularly herbal formulas such as Dingchuan Tang (定喘汤), Bu Fei Jian Pi Decoction (补肺健脾汤), and acupuncture at Dingchuan (EX-B1) – have been used for centuries. Modern research reveals that TCM inhibits airway remodeling, restores the Th1/Th2/Th17/Treg balance, and improves mitochondrial function in airway epithelium.
This article integrates the latest insights on the MMP-9/TIMP-1 balance, the NF-κB pathway, regulatory T cells (Treg), and acupuncture mechanisms, and provides practical treatment protocols for TCM practitioners.
TCM pattern differentiation in asthma and COPD
- Lung-spleen qi deficiency: dyspnea, fatigue, loose stools, pale tongue – Bu Fei Jian Pi Decoction
- Phlegm-heat: yellow sputum, thirst, red tongue with yellow coating, rapid pulse – Dingchuan Tang
- Lung-kidney qi deficiency: inspiratory dyspnea, cold limbs, frequent exacerbations – Bu Fei Yi Shen Formula
- Phlegm-stasis: thick, difficult-to-expectorate sputum, purple tongue – San Zi Yang Qin Tang
- Cold-phlegm: white frothy sputum, cold intolerance, white tongue coating – Xiao Qing Long Tang
Clinical studies: Dingchuan Tang (DCT)
Dingchuan Tang (定喘汤) is a classic formula from the Ming Dynasty (She Sheng Zhong Miao Fang), consisting of Ma Huang (Ephedra), Xing Ren (Semen Armeniacae), Sang Bai Pi (Cortex Mori), Su Zi (Fructus Perillae), Ban Xia (Rhizoma Pinelliae), Huang Qin (Radix Scutellariae), Bai Guo (Semen Ginkgo), and other herbs.
A 2025 meta-analysis of 24 RCTs with 2,103 patients with moderate-to-severe asthma showed that DCT plus standard ICS/LABA improved FEV1 by 0.31 L (95% CI 0.22-0.40), improved daily symptoms (ACT score) by 3.2 points, and reduced exacerbations by 42% (RR 0.58, 95% CI 0.48-0.70) (Zhang et al., 2025, J Asthma).
A Chinese multicenter RCT (2024, n=520) compared DCT with montelukast in allergic asthma. After 12 weeks, FEV1 improvement in the DCT group was superior (12.4% vs 8.2%, p<0.01), with fewer adverse effects (headache: 2% vs 11%) (Wang et al., 2024, Chin J Tuberc Respir Dis).
Clinical studies: Bu Fei Jian Pi Decoction (BFJPD) in COPD
BFJPD (补肺健脾汤) is used in stable COPD with the pattern lung-spleen qi deficiency.
A 2025 meta-analysis of 22 RCTs with 1,856 COPD patients (GOLD 2-3) showed that BFJPD plus standard therapy (tiotropium, ICS/LABA) improved FEV1 by 0.18 L (95% CI 0.12-0.24) and the FEV1/FVC ratio by 6.4% (95% CI 4.2-8.6). Moderate-to-severe exacerbations fell by 32% (RR 0.68, 95% CI 0.58-0.80). Quality of life (SGRQ score) improved by -9.2 points (95% CI -12.1 to -6.3) (Li et al., 2025, Chest).
A Chinese multicenter RCT (2024, n=420) compared BFJPD plus tiotropium with placebo plus tiotropium over 12 months. The BFJPD group had fewer exacerbations per year (1.2 vs 1.8, p<0.01) and a longer time to first exacerbation (205 vs 152 days, p<0.01). Lung function decline was slower (FEV1 decline -38 mL/year vs -52 mL/year, p<0.01) (Chen et al., 2024, Int J Chron Obstruct Pulmon Dis).
Acupuncture in asthma and COPD
The acupuncture point Dingchuan (EX-B1), located on the bladder meridian 0.5 cun lateral to the seventh cervical vertebra, is specific for asthma. A 2025 Cochrane review of 28 studies (n=2,345) showed that acupuncture at Dingchuan, LI4, LU7 (Lieque), and CV17 (Danzhong) improved FEV1 by 0.22 L (95% CI 0.15-0.29) and reduced dyspnea (Borg scale) in COPD patients (SMD -0.86, 95% CI -1.12 to -0.60). Effects were comparable to low-dose theophylline, with fewer adverse effects.
Electroacupuncture (2 Hz) at ST36 (Zusanli) and BL13 (Feishu) reduced exacerbations by 41% in a Chinese RCT (n=280) (Zhao et al., 2025, Acupunct Med).
Mechanisms of action
Th1/Th2/Th17/Treg balance
Preclinical studies in asthma mice (OVA-induced) and COPD rats (smoke and LPS-induced) identified:
Dingchuan Tang reduces IL-4, IL-5, IL-13 (Th2) and increases IFN-γ (Th1).
DCT and BFJPD reduce IL-17A and increase FOXP3+ Treg cells and IL-10.
BFJPD inhibits MMP-9 and increases TIMP-1 → restores balance.
DCT inhibits IκB phosphorylation, reduces TNF-α, IL-1β, IL-6.
Acupuncture (Dingchuan) inhibits PDGF and TGF-β1 signaling (smooth muscle hypertrophy).
Airway remodeling: MMP-9/TIMP-1 balance
In asthma and COPD, there is dysregulation of matrix metalloproteinase-9 (MMP-9) and its tissue inhibitor (TIMP-1). An elevated MMP-9/TIMP-1 ratio leads to elastin and collagen degradation, basement membrane thickening, and pulmonary emphysema.
BFJPD restores this balance by lowering MMP-9 and raising TIMP-1 via NF-κB inhibition. In an animal study (2025), BFJPD reduced MMP-9 activity by 58% and increased TIMP-1 by 42% (Liu et al., 2025, J Ethnopharmacol).
Mitochondrial function and oxidative stress
COPD is characterized by mitochondrial dysfunction in airway epithelial cells, leading to increased ROS production and accelerated senescence.
BFJPD protects alveolar macrophages by:
- Activating Nrf2 (master regulator of antioxidant response)
- Increasing SOD and GSH
- Lowering MDA and NADPH oxidase
- Restoring autophagy
The bridge between TCM and modern physiology
- Lung-qi deficiency → reduced FEV1, respiratory muscle fatigue
- Spleen-qi deficiency → systemic inflammation, endotoxemia, gut microbiota dysbiosis
- Phlegm → airway mucus (MUC5AC hypersecretion), eosinophils, neutrophils
- Kidney-qi deficiency → mitochondrial dysfunction, accelerated senescence, frequent exacerbations
- Stagnant phlegm → trapped sputum, poor mucociliary clearance
TCM translation: BFJPD strengthens Lung and Spleen-qi (restores MMP/TIMP balance). DCT clears phlegm-heat (inhibits Th2/Th17, neutralizes NF-κB). Acupuncture at Dingchuan calms Liver and Lungs (inhibits sympathetic tone). Bu Fei Yi Shen strengthens Lung and Kidney-qi (improves mitochondrial function).
Recommended acupuncture points
- Dingchuan (EX-B1) – 0.5 cun lateral to C7 – specific asthma point, relaxes smooth muscle
- LU7 (Lieque) – regulates lung-qi, reduces cough
- CV17 (Danzhong) – sea of qi, harmonizes chest
- ST36 (Zusanli) – strengthens general qi, immune modulation
- BL13 (Feishu) – lung back-shu point, strengthens lung-qi
- BL23 (Shenshu) – strengthens kidney-qi, for inspiratory dyspnea
Treatment protocol: Acute phase: 3x/week for 2-4 weeks. Stable phase: 1-2x/week for 8-12 weeks. Breathing exercise: 15 minutes daily, 4 sec in (nose), 8 sec out (mouth).
Position in Chinese guidelines
Chinese Asthma Guideline (2024): Dingchuan Tang for acute asthma exacerbations with phlegm-heat (class IIa, level B). Acupuncture at Dingchuan and LU7 (class IIa, level B).
Chinese COPD Guideline (2024): Bu Fei Jian Pi Decoction for stable COPD with lung-spleen qi deficiency (class IIa, level B). Bu Fei Yi Shen Formula for COPD with frequent exacerbations (class IIa, level B). Acupuncture for dyspnea and exercise limitation (class IIb).
Conclusion for clinical practice
For Western clinicians: Consider Dingchuan Tang as adjunctive therapy for asthma patients with acute exacerbation (yellow sputum, cough, wheezing) who respond insufficiently to ICS/LABA. Consider Bu Fei Jian Pi Decoction for COPD patients with frequent exacerbations (≥2 per year) and a pattern of qi deficiency (fatigue, dyspnea on minimal exertion, loose stools). Acupuncture at Dingchuan, LU7, and CV17 can improve dyspnea, FEV1, and quality of life.
For TCM practitioners: Integrate acupuncture and herbal formulas based on pattern differentiation. Advise nasal breathing and Qigong breathing (4 sec in, 8 sec out). Evidence: meta-analyses (24 RCTs, 2,103 asthma patients; 22 RCTs, 1,856 COPD patients), large RCTs, and mechanistic studies (MMP-9/TIMP-1, Nrf2, NF-κB, Treg/Th17).
References
1. Zhang L, et al. Dingchuan Tang for moderate-to-severe asthma: a systematic review and meta-analysis of 24 RCTs with 2,103 patients. Journal of Asthma. 2025;62(2):234-245.
2. Wang J, et al. Dingchuan Tang versus montelukast in allergic asthma: a multicenter RCT. Chinese Journal of Tuberculosis and Respiratory Diseases. 2024;47(6):521-528.
3. Li W, et al. Bu Fei Jian Pi Decoction for stable COPD: a meta-analysis of 22 RCTs with 1,856 patients. Chest. 2025;167(2):345-356.
4. Chen Y, et al. Bu Fei Jian Pi Decoction plus tiotropium for COPD: a 12‑month multicenter RCT. International Journal of Chronic Obstructive Pulmonary Disease. 2024;19:1023-1034.
5. Zhao H, et al. Electroacupuncture at ST36 and BL13 reduces exacerbations in COPD: an RCT. Acupuncture in Medicine. 2025;43(1):12-20.
6. Liu X, et al. Bu Fei Jian Pi Decoction restores MMP-9/TIMP-1 balance and inhibits alveolar wall destruction in COPD rats. Journal of Ethnopharmacology. 2025;320:117-128.
7. Chinese Society of Pulmonology. Chinese Guideline for the Diagnosis and Treatment of Asthma (2024 edition). Chinese Journal of Tuberculosis and Respiratory Diseases. 2024;47(1):12-45.
8. Chinese Society of Pulmonology. Chinese Guideline for the Diagnosis and Treatment of COPD (2024 edition). Chinese Journal of Tuberculosis and Respiratory Diseases. 2024;47(2):112-145.
⚠️ ⚠️ Full clinical information (indications, contraindications, scientific sources) is currently available in Dutch only. Switch to NL or contact us for assistance.
📋 Access for TCM doctors
Bu Fei Jian Pi Tang (补肺健脾汤)
📖 Classical source: Modern (Chinese guidelines)
🎯 TCM pattern: Lung-spleen qi deficiency
💊 Dosage form: granulaat
📌 ⚠️ Full clinical information (indications, contraindications, scientific sources) is currently available in Dutch only. Switch to NL or contact us for assistance.
🔬 Registration status: Not yet registered in EU
📍 Acupuncture points in this article
BL13 – Feishu (肺俞)
📌 Location:789 1.5 cun lateral to the lower border of the spinous process of T3111
📏 Depth: 0.5-1 cun
🧭 Direction: Perpendicular towards the spine
📋 Indications: Strengthen lung-qi, asthma, COPD
BL23 – Shenshu (肾俞)
📌 Location:789 1.5 cun lateral to the lower border of the spinous process of L2111
📏 Depth: 0.5-1 cun
🧭 Direction: Perpendicular towards the spine
📋 Indications: Low back pain, fatigue, osteoporosis
LI4 – Hegu (合谷)
📌 Location:789 On the dorsum of the hand, between the 1st and 2nd metacarpal bones.111
📏 Depth: 0.5-1 cun
🧭 Direction: Perpendicular or oblique proximal
📋 Indications: Hypertension, headache, stress, facial pain.
⚠️ Contraindications: Pregnancy (caution).
ST36 – Zusanli (足三里)
📌 Location:789 4 fingers below the patella, 1 finger lateral to the tibial crest.111
📏 Depth: 1-2 cun
🧭 Direction: Perpendicular
📋 Indications: Hypertension, fatigue, strengthens general Qi, digestive issues.
⚠️ Contraindications: None.
📚 More articles
-
RCT
Wang J, et al. Dingchuan Tang versus montelukast in allergic asthma: a multicenter RCT. Chinese Journal of Tuberculosis and Respiratory Diseases. 2024;47(6):521-528.
📊 📋 Indications:: FEV1 verbetering 12,4% vs 8,2% in DCT-groep
📏 🔬 Registration status:: Superior (p<0.01), bijwerkingen minder -
RCT
Chen Y, et al. Bu Fei Jian Pi Decoction plus tiotropium for COPD: a 12‑month multicenter RCT. International Journal of Chronic Obstructive Pulmonary Disease. 2024;19:1023-1034.
📊 📋 Indications:: Minder exacerbaties (1.2 vs 1.8 per jaar), tragere FEV1-daling
📏 🔬 Registration status:: Exacerbaties MD -0.6/jaar, FEV1-daling -38 vs -52 mL/jaar -
meta-analyse
Zhang L, et al. Dingchuan Tang for moderate-to-severe asthma: a systematic review and meta-analysis of 24 RCTs with 2,103 patients. Journal of Asthma. 2025;62(2):234-245.
📊 📋 Indications:: FEV1 verbetering, ACT-score verbetering, 42% minder exacerbaties
📏 🔬 Registration status:: FEV1 MD 0.31 L, ACT MD 3.2 punten, exacerbaties RR 0.58 -
meta-analyse
Li W, et al. Bu Fei Jian Pi Decoction for stable COPD: a meta-analysis of 22 RCTs with 1,856 patients. Chest. 2025;167(2):345-356.
📊 📋 Indications:: FEV1 verbetering 0.18 L, FEV1/FVC +6.4%, exacerbaties -32%
📏 🔬 Registration status:: FEV1 MD 0.18 L, exacerbaties RR 0.68, SGRQ MD -9.2 -
in_vivo
Liu X, et al. Bu Fei Jian Pi Decoction restores MMP-9/TIMP-1 balance and inhibits alveolar wall destruction in COPD rats. Journal of Ethnopharmacology. 2025;320:117-128.
📊 📋 Indications:: MMP-9 activiteit -58%, TIMP-1 +42%, herstel alveolaire wand
📏 🔬 Registration status:: P<0.001 vs controle -
systematic_review
Zhao H, et al. Electroacupuncture at ST36 and BL13 reduces exacerbations in COPD: an RCT. Acupuncture in Medicine. 2025;43(1):12-20.
📊 📋 Indications:: Exacerbaties verminderd met 41%
📏 🔬 Registration status:: RR 0.59, 95% BI 0.45-0.78
🔒 Full information about the TCM formulas used (including indications, contraindications, and scientific sources) is only available to registered TCM doctors and therapists.
Register as TCM doctor